
By Palmer R. Cook, OD






A successful matching of prescription, eyewear and patient is a three-way marriage which yields the outcome intended by the doctor and expected by the patient. Patients usually want and anticipate improved vision and an improved appearance. Additionally, the fit of the eyewear should work well and be comfortable. ECPs face these challenges daily, and they are often difficult to meet.
The task of choosing just the right frame for new lenses can be a daunting challenge in itself. Appearance, function, comfort as well as value/cost are related issues, and the relative importance of each varies from patient to patient. Lens thickness, weight and performance are factors that are impacted by the frame choice to a much greater extent than those outside the profession realize. Weight, peripheral aberrations, magnification/minification and unwanted prism-related effects can be reduced (or increased) by the careful or not-so-careful process of frame selection.
The patient’s facial anatomy plays an important role in nearly every aspect of finding the best frame/lens combination. And of course, the parameters of the prescription must be scrupulously met.
It is important to realize that every patient ordering new eyewear has been through a seemingly puzzling series of objective and subjective tests. In our society, buying and selling becomes a part of everyone’s experience at an early age. Upon seeing frames on display, patients are inclined to think, “At last here is something I can understand,” and as every ECP knows, they couldn’t be more mistaken.
ESTABLISH YOUR CREDIBILITY
To create really satisfying eyewear, the frame stylist/optician and patient must work together. It is imperative for the patient to have confidence in the optician as a professional guide. Otherwise, outcomes can range from disappointing to disastrous, and a great deal of time and effort may be wasted in just preventing inappropriate choices.
The best way for the optician to establish his or her professional role in the dispensary is to start the eyewear discussion with the prescription and lenses. That discussion should include at least a mention of what the doctor feels works best for that particular kind of prescription.
Most people purchasing new eyewear are unaware of the importance of lens options and alternatives. After all, they have a prescription, the lenses have been doctor-specified, so only that and nothing more is often in their thinking. All experienced ECPs understand that mindset because it is so common and so problematic.
Lightweight lenses, low reflectance lenses, no-line lenses, cosmetically tinted lenses, ultra-thin lenses and low curvature lenses are available just to name a few options that can improve the performance, appearance and comfort of the eyewear’s outcome. Finding the “best” frame is closely related to the kind of lenses that are ideal for your patient’s needs, so a discussion regarding lens materials and lens designs should be initiated before starting the frame selection. It is a good idea to mention anti-reflective properties and UV blocking since they can improve the appearance and performance of their prescription.
Patients also need to be aware that although many frames may appear to be very similar, some are specifically designed for particular kinds of prescriptions. A key purpose of a short preliminary discussion is to help the patient recognize the complexity of getting the best possible outcome.
APPEARANCE
Children, teens, adults and seniors all tend to approach frame selection with one thought in common: How can I find one that will look best on me? Below are some guidelines to help in creating eyewear that not only looks good, but functions as it should and does so with comfort.
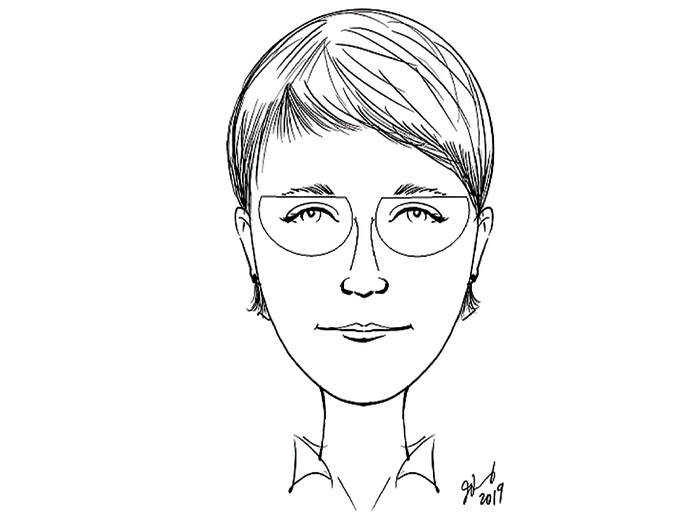
- Eyewear should be about as wide as the widest part of the face (Fig. 1). Nonnie’s frame violates the “as wide as the widest part of the face” guideline, but the BO prism in the lateral periphery of each lens will cause an unsightly facial inset if the frame is too wide. Her relatively narrow PD would be more obvious in larger lenses. The abrupt nasal upsweep of the lenses tends to minimize her narrow-nose appearance. A roll and polish would help address her concern about edge thickness.
Although Nonnie doesn’t need an add, digital atoric SV lenses would give her a wider binocular “sweet spot.” She is a keen observer, and she would appreciate the performance and cosmetic advantages of anti-reflective lenses. She will understand the importance of a second pair which could also help her color-coordinate her eyewear with her wardrobe.
The eyes should center a little more than halfway from the bottom of the lens to the top of the lens after the frame is properly adjusted.
- Generally, frames should follow the line of the eyebrows, and the top of the front should be at about the level of, or slightly below, the eyebrows.
- If the patient has heavy eyebrows and strong facial features (Fig. 2), thicker, darker frames usually work best.
- Frames that are short from top to bottom (i.e., short B measurement—sometimes called big difference frames) elongate the face. Frames that have longer B measurement (i.e., a small difference frame) tend to shorten the face.
- A high bridge attachment to the eyewires will lengthen a short nose. Paul’s high bridge (Fig. 3) and relatively short B measurement helps lengthen his nose. Using an oval shape helps achieve a blended look for Paul. His wide bridge and adjustable pads allow an adjustment that gives better air circulation to reduce fogging. His temple attachments are halfway from the top to the bottom of the eyewires, and the lenses will pivot around a horizontal axis when pantoscopic tilt is added. This reduces the inward swing of the bottom of the lenses by half, compared to a frame with the same B measurement with a temple attachment at the top of the lenses. The low temple attachment will help relieve the riding of the frame on his cheeks when Paul smiles, and it will also help reduce the lens fogging.
- A low bridge attachment tends to disguise a long nose. John (Fig. 2) has a bridge attachment just above the datum line, which helps reduce the apparent length of his long nose.
- High power prescriptions work better in oval and rounded shapes because they will have thinner edges in minus powers and less center thickness (and less magnification) in plus powers. Also, areas in the far periphery of high powered lenses have annoying aberrations, so patients in the high prescription ranges become head-turners in order to use the best performing area of their lens as much as possible. The lens areas eliminated by an oval or round shape in place of a more rectangular are seldom missed when the Rx is in the medium or higher power range.
- Decentering the MRPs of SV and lined lenses as well as the Fitting Crosses of PALs from 1 mm to 3 mm is a good rule for best lens performance and easier adaptation. Keeping the patient’s monocular PDs in mind during frame selection can help avoid later problems. Lenses should never be decentered outward.
- The pantoscopic angles are the angles each temple makes with the plane of the front. They will differ if one ear is anatomically higher than the other. It is a good idea to guide these patients away from “wide temple” styles which do not accept changes of the pantoscopic angles.
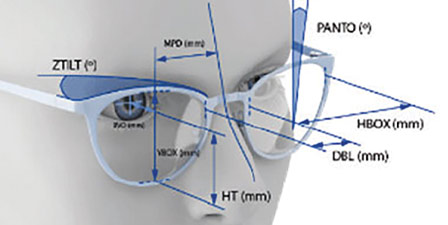
- Pantoscopic tilt is the rotation of the lens plane relative to the horizontal line-of-sight around a horizontal axis. This causes the lower portion of a vertical lens to move closer to the face. Using an inclinometer or a smartphone with a “level” app makes it easy to establish head tilt and measure pantoscopic tilt when ordering “as worn” lenses.
AS WORN LENS TECHNOLOGY
The power of a lens varies depending on its distance from the eye. This effect is well understood by all experienced ECPs. A lesser recognized effect is that if a lens is tilted around a vertical or a horizontal axis (or a combination of both) significant unwanted lens power changes cylinder, and prism may be created. With digital lens technology, it became practical to make ophthalmic lenses that match the powers determined in an eye examination. These individualized lenses could be compared to tailored suits as opposed to off-the-rack clothing.
Eye exams utilize lenses that lay in a plane perpendicular to the patient’s line-of-sight. When the lenses are mounted in frames, the effective power changes, and prism is added. These can be neutralized by using digitally produced lenses. Such lenses are referred to as “individualized,” “as worn” or “compensated” because even though they are tilted or wrapped when worn, they accurately give the precise power intended by the prescribing doctor. Patient sensitivity varies widely, but particularly for the mid-range powers and higher, this is a hugely promising step forward.
To alleviate ECP concerns about correctly measuring when using individualized lens technology, manufacturers offer “default measurements.” Labs report that nearly all orders for individualized lenses are now received with the default measurements. This leads to unfortunate outcomes, because unless the patient matches those measurements, the lenses will not be individualized for the patient who paid for that excellent technology. Measuring the vertex, wrap and pantoscopic tilt is not difficult, and using those measurements (even though they may be slightly in error) is better than using average findings established by people who have never seen your patient.
Fitting Mirrors—It is natural for patients to move closer to the mirror to try to get a good look at the frame they are considering. They will have a better perception of the frame’s appearance if they move back from the mirror. Let your patients know that people who see them will not move to within inches of their face to examine their eyewear. People tend to notice new eyewear and whether it complements appearance from a distance of 10 feet or more.
Concave mirrors give a magnified view, but they can be a fire hazard if sunlight is reflected and focused on upholstery or drapes. Convex mirrors minify and are not very useful for dispensary purposes. A full-length mirror is helpful in evaluating the effect of one or another frame depending on the patient’s refractive error. Non-reversing mirrors are available that let patients get a facial view so they can see themselves “as others see them.” Electronic mirrors with varying degrees of sophistication are available and can be seen at the major trade shows. Simply using your phone to snap a photo to be shown on the phone screen or a larger screen is a non-mirror option to help your patient make a decision.
FACIAL SHAPE AND FRAME SELECTION
Some faces are angular, some are curved. Curved facial shapes include round, oval, heart and inverted heart. Angular facial shapes include square, rectangular, triangular, inverted triangular and diamond. Variations on these basic shapes seem infinite. For a “blended look,” consider more rounded frames for patients with a curved facial shape. Frames shaped with corners are usually more appropriate if the facial shape is angular.
For a “balanced look,” frames that soften extremes in the facial anatomy are used, while a dramatic look tends to exaggerate those extremes. Unusual frame styles are sometimes used to create a dramatic or iconic look by politicians, actors or others who are in the media. Most patients prefer a “blended design” which blends with their facial anatomy.
Polly (Fig. 4) has an inverted heart facial shape. Polly’s most attractive features are her eyes and dark brick-red hair. She makes a fashion statement with her delicate green enameled frame and fashion-tinted green lenses, which call attention to both of her best features. Her frame is a 52o16. Her PD is 29/32, giving her a decentration OD of 5 mm and OS 2 mm. Polly’s Rx is in the higher plus range so the excessive decentration of the right lens will give a substantially greater nasal edge thickness and center thickness of the lens. The increase in magnification due to the increased center thickness could be cosmetically undesirable because of preferentially magnifying her right eye. This will be exaggerated if she has a long vertex distance. Issues of adaptation and spatial orientation related to an induced aniseikonia could also occur. Increasing the index to flatten and thin the lenses may help significantly.
Because Polly drives into the sun going to and returning from work, she will appreciate the suggestion of having top quality driving eyewear for her daily commute. That is particularly true during the months in which the sun hangs low in the sky at sunset and sunrise.
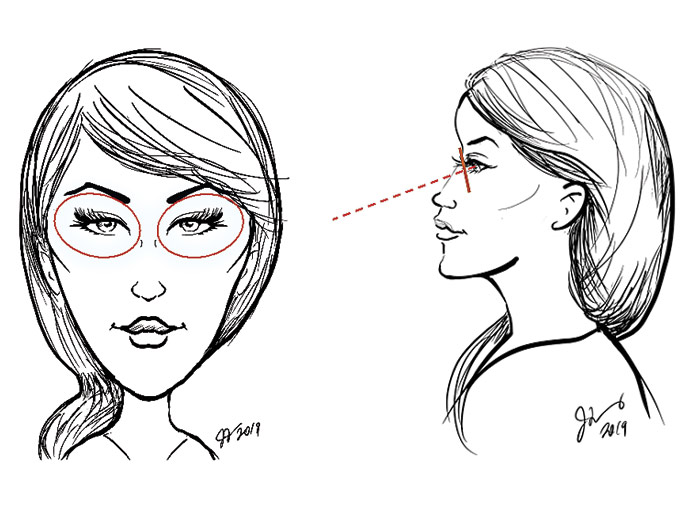
LASH RELIEF
The move to flatter, thinner lenses that came with the digital lens revolution certainly has its benefits, but one less positive issue is the reduction of lash relief for some patients. Priscilla (Fig. 5) is an example. Viewed in profile with the eyewear properly adjusted, the ECP has asked Priscilla to keep her chin up as though she was looking at the horizon. Then the ECP held her thumb up as a target at reading distance and on Priscilla’s mid-line. She then slowly raised and lowered her thumb-target until she found the position at which Priscilla’s long lashes extended straight out. This technique makes the lash relief issue easy to evaluate.
Corrected curve lenses should be used for Priscilla because their greater sag depth helps give more lash relief. Increasing the lens curvature is more effective if larger lenses are used because this further increases their sag depth. In no case should the lenses just be given some arbitrarily chosen steeper curve. In cold weather, new plastic lenses can develop a static electricity charge, and even though the lashes are not touching, an annoying sensation of touching can occur due to static electricity. Using a good quality AR with anti-stat properties may reduce that sensation.
If Priscilla’s Rx is in the minus range, the apex of the bevel may be moved posteriorly, and that will move the lens a bit further from her eyes. Labs often term this a 1/3 – 2/3 bevel placement. Adjustable pads also will allow a further increase in Pricilla’s lash relief. Priscilla should understand that everything possible will be done to prevent her lashes from contacting the lens, but if worse comes to worse, the lashes can be trimmed shorter. This is an option that generally makes using the lens curler and/or refraining from lash extender options suddenly more acceptable.
Young children sometimes have lashes a centimeter or more long. Because they often have noses with underdeveloped bridges and eyewear with small diameter eyewires, lash relief can be a problem. Building up the nosepads of a zyl bridge and reducing any frame wrap can be helpful.
Most eye exams are performed with the refractor carefully leveled, but sometimes eyewear looks best if the frame is tilted (Fig. 2). For patients with cylinder, this frame tilt changes the axis of the cylinder and also may induce unwanted vertical prism. Consulting the prescribing doctor is a good idea when eyewear will look best rotated from the leveled position of the refractor as it is typically used in the exam.
Hyper eye patients, such as John in Fig. 2, are sometimes inadvertently diagnosed as needing vertical prism, because testing was done with the patient’s eyes at different levels as they peered through the refractor. These patients often report a history of significant difficulty in adapting to new eyewear.
APPEARANCE, FUNCTION AND COMFORT
You are challenged daily with balancing Appearance, Function and Comfort. Take a few moments to review the prescription and look at your patient carefully before you start. Listen to what he or she has to say about previous eyewear. Whether you hear the good, the bad or the ugly, what you hear can help you. Understand the advantages and limitations of today’s modern ophthalmic technologies.
Today’s technologies are better than ever, but just as with medications, their correct applications must be understood if you are to use them well. Eyewear design is a mixing of art, science and an understanding of human psychology. That’s a learning curve that never ends. Boost that curve by regularly monitoring your outcomes as part of your regimen of providing the very best in eyecare.■
Contributing editor Palmer R. Cook, OD, is an optometric educator and optical dispensing expert. Special thanks to Joni Fleming for converting word descriptions of our supporting cast of Paul, John, Polly, Pricilla and Nonnie into caricatures for a little fun with the art, science and psychology of ophthalmic optics.